How to interpret an ECG: guide for healthcare professionals
Interpreting the ECG consists of a number of parameters important for an informed clinical decision. Let us take a look at the most vital aspects of ECG interpretation – from distances on the ECG paper to the intricacies of waves, waveforms, segments, and intervals. We will also discuss how to interpret duration and the data on cardiac axis.
A big role in ECG interpretation is also played by automatic algorithms. When an ECG is recorded using a machine equipped with the Glasgow Interpretation Algorithm, the collected data is processed and analyzed by it. The algorithm takes into account a variety of patient-specific factors, such as age, gender, race, and clinical history, to provide a more accurate and tailored interpretation of the ECG results.
In this blog you will learn:
Distances on ECG paper or graph
Waves
Waveforms
Segments
Intervals
Duration
Axis
Automatic interpretation
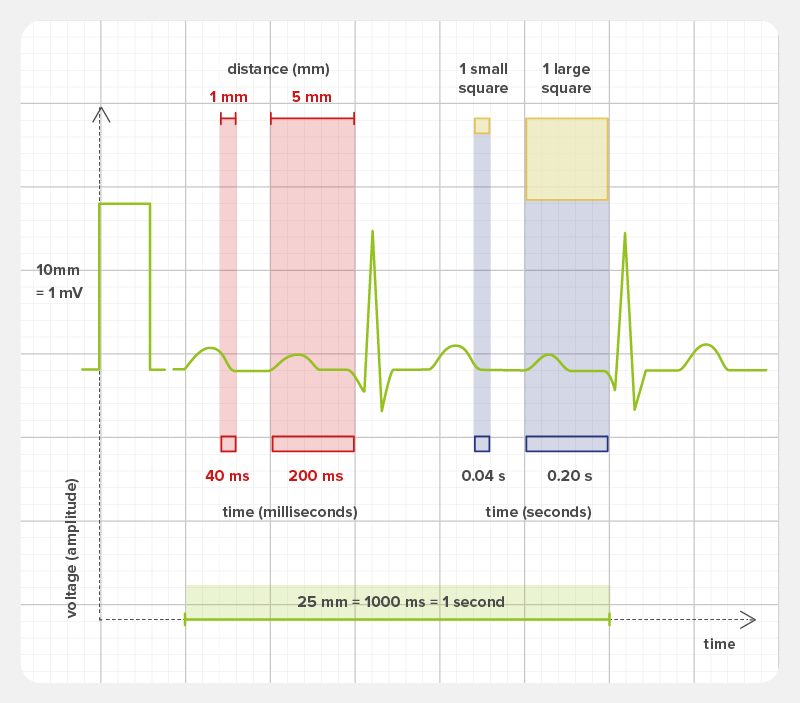
Distances on ECG paper or graph
The ECG paper, divided into squares, shows the passage of time during ECG measurement on the rhythm strip.
The standard paper speed is 25 mm/s. The rhythm strip is comprised of:
1 SMALL square (1 mm) = 0.04 s (40 ms)
5 SMALL squares (5 mm) = 1 LARGE square = 0.2 s (200 ms)
5 LARGE squares = 1 second
250 SMALL squares = 50 LARGE squares = 10 seconds
Waves
The electric activity of the heart, as captured by the ECG leads, is shown in the form of waves. One heartbeat (i.e. one cardiac cycle) consists of a number of waves. For a medical interpretation, the following waves and their combinations are considered. [3]
Individual waves
Individual waves in the ECG are the following:
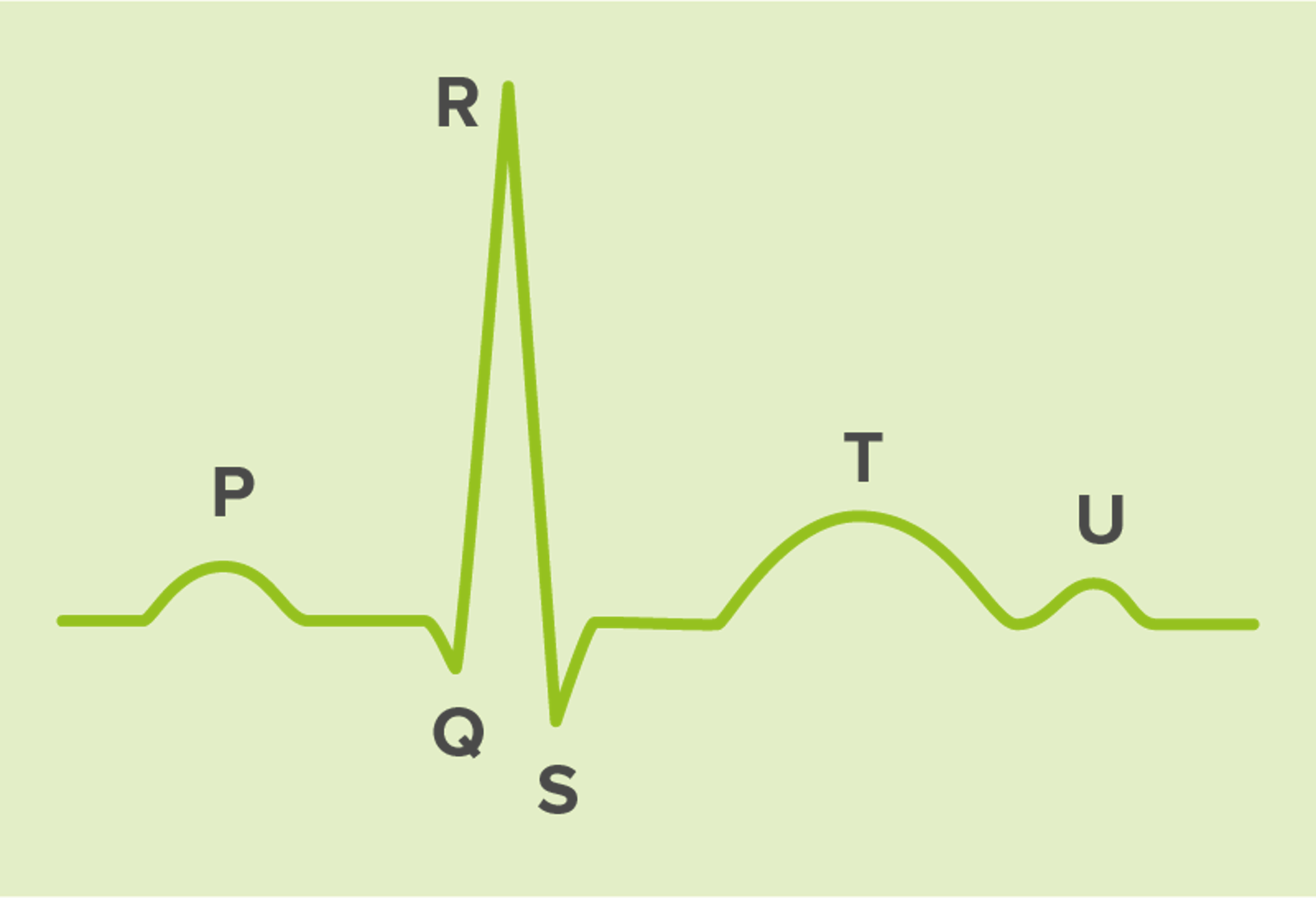
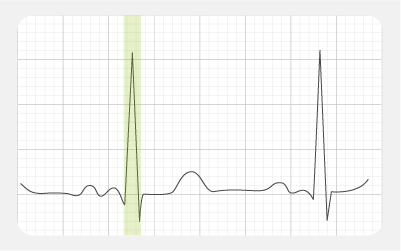
- R wave: reflects depolarisation of the main mass of the ventricles.
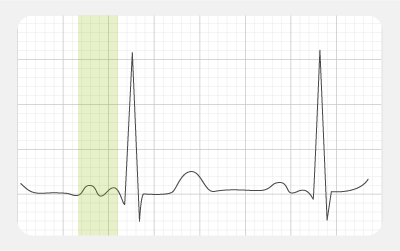
- P wave: represents atrial depolarisation.
- Q wave: represents the normal left-to-right depolarisation of the interventricular septum.
- S wave: signifies the final depolarisation of the ventricles.
- T wave: represents ventricular repolarisation.
- U wave: a small, rounded deflection sometimes detected after the
- T wave: It represents the last phase of ventricular repolarisation, but its exact source remains unclear.
Wave combinations
ECG waves can be joined into various combinations, each of which gives us additional information about the patient’s heart cycle:
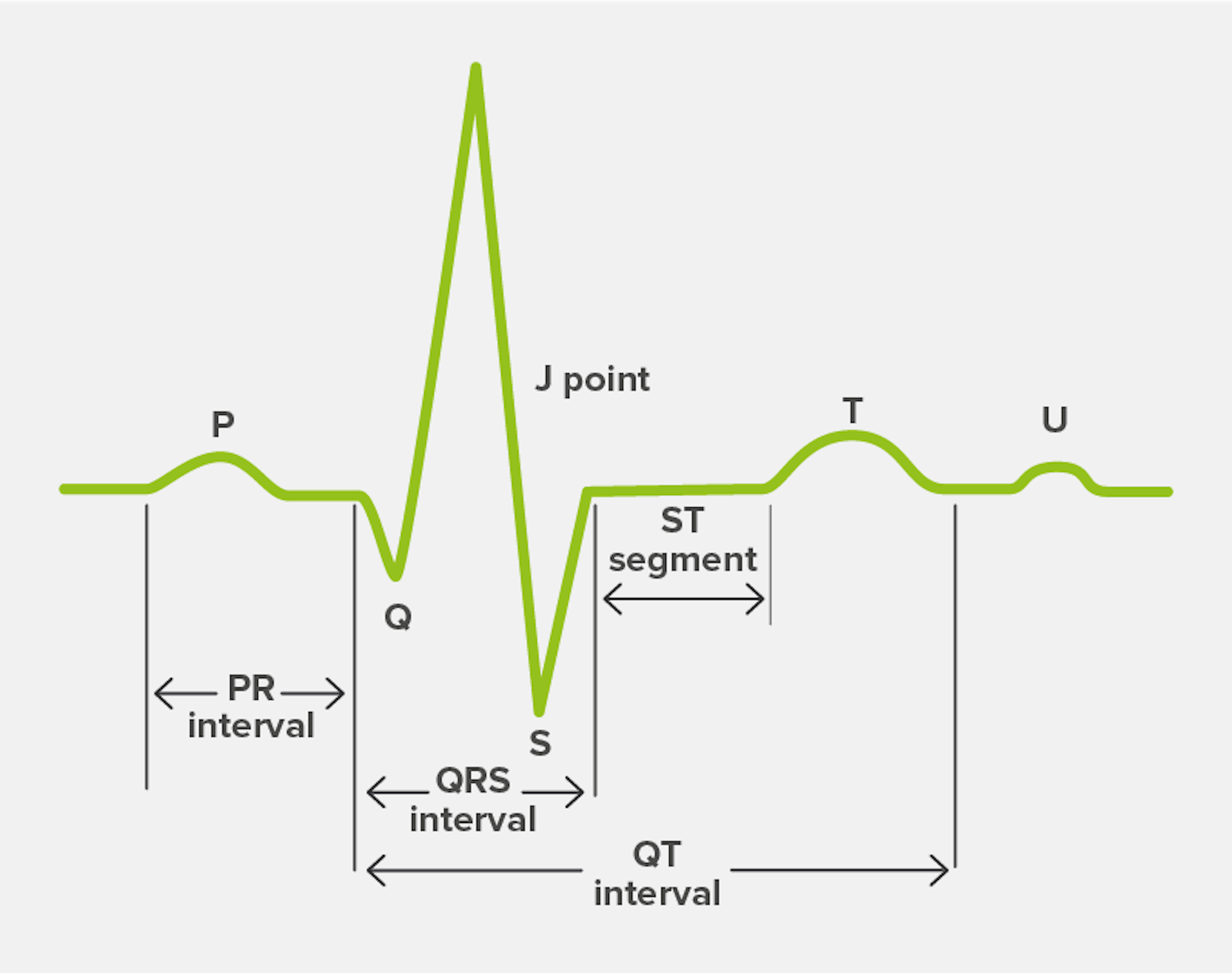
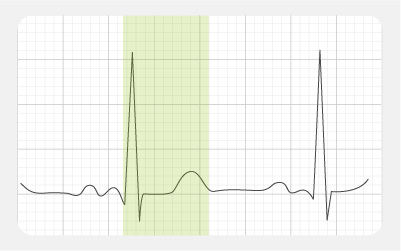
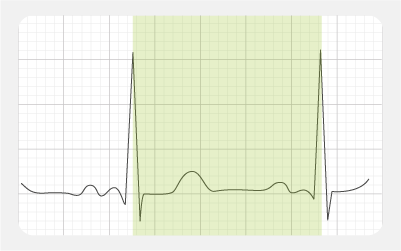
- PR interval: the time from the beginning of atrial depolarisation to the beginning of ventricular depolarisation
- QT interval: the time from the beginning of ventricular depolarisation to the end of ventricular repolarisation
- QRS interval: the time from the beginning to the end of ventricular depolarisation
- ST segment: the time from the end of ventricular depolarisation to the beginning of ventricular repolarisation
- J point: where the QRS complex and the ST segment connect (important e.g. when distinguishing between acute cardiac ischemia from a normal variant)
Waveforms
Waves have a variety of characteristics. [2] They include:
Duration
(Example: an unusually long P wave may be a sign of left atrial enlargement. Normal: =< 0,12 s)

Amplitude
(Example: an unusually tall P wave may be a sign of right atrial enlargement. Normal: < 2,5 mm)
Morphology
(Example: an inverted P wave may indicate an origin of a heart rhythm other than a sinus node)

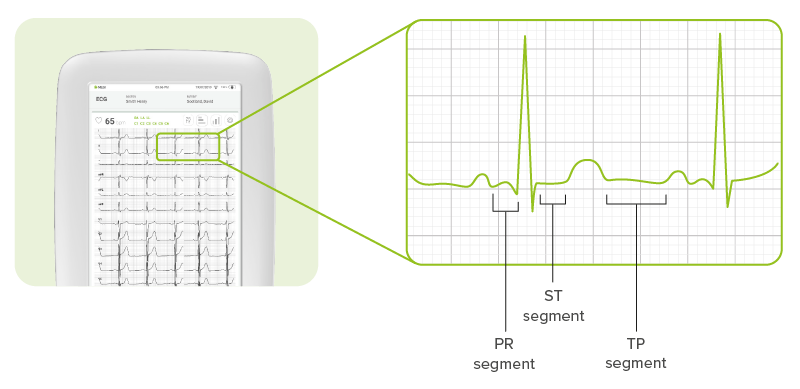
Segments
Segments are the lines that connect the waves:
PR segment connects P wave and QRS complex
ST segment connects QRS complex and T wave
TP segment line connects the T wave with the following P wave
Intervals
PR interval is the sum of the duration of the P wave + the PR segment
QRS interval is the duration of the QRS complex
QT interval = duration of QRS complex + ST segment + T wave
RR interval = duration of all waveforms and segments within one cardiac cycle
Duration
| Interval | Normal duration | Significance of abnormal duration |
|---|---|---|
| PR | 120-200 ms | < 120 ms: abnormal connection between atria and ventricles >200 ms: delayed conduction through AV node |
| QRS | =< 120 ms | > 120 ms: abnormail sequence of ventricular deplorisation, or excessive ventricular mass |
| QT | =< 1/2 RR interval (on approximation) | > 1/2 RR interval: delayed ventricular repolarisation |
| RR | 600-1000 ms (HR: 600-100 bpm) | > 100 bpm: tachycardia < 60 bpm: bradycardia |
Note: Tachycardia and bradycardia do not necessarily indicate pathology; a lot depends on the patient’s age and condition.
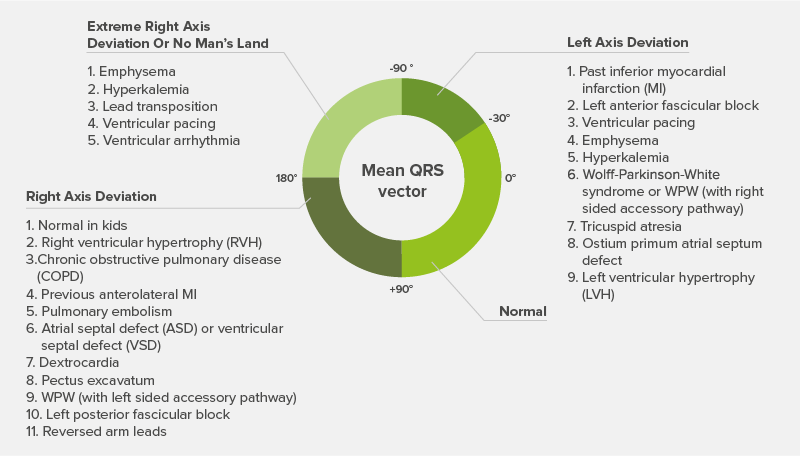
Axis
The cardiac axis gives us an idea of the overall direction of electrical activity, and its deviation to either left or right can indicate various conditions. [5]
Automatic interpretation Algorithm
Introduction to the Glasgow Interpretation Algorithm
The Glasgow ECG Interpretation Algorithm, developed at the University of Glasgow, UK, enables automatic ECG analysis. The algorithm has been in continuous development for over 30 years. [6]
It has been adapted to meet the needs of different patients (the algorithm accounts for age, gender and race and compares the ECG with historic data to arrive at specific interpretations). It is applicable to neonates as well as adults and takes account of racial variation in wave amplitudes.
How the algorithm works
The University of Glasgow (Uni-G) ECG interpretation program is based on an analysis of simultaneously recorded leads acquired at 500 samples per second. [7]
The first stage in analysis is to apply a 50 Hz or 60 Hz notch filter to remove AC interference. Then, it checks if there are any errors in the recording of any of the leads. If there are, it replaces that part of the recording with one continuous value, or the lead may be set as unavailable if too noisy.
Next, the program identifies the QRS complex and determines its type. In simple terms, this is done by comparing the first complex in Lead I with the second complex in the same lead, and then comparing all the complexes in this lead. The process is repeated for four other leads, as usually just one or two leads will show aberrations in the conducting of the complex.
A complex selection procedure then decides which heartbeat will be selected for averaging and subsequent interpretation.
The advantages of the Glasgow ECG Interpretation
While other products use only age and gender to a limited extent, the Glasgow Algorithm uses more clinically significant variables. They are gender, age, race, and clinical history. This is critical because ECG patterns for patients of various ages from different ethnic backgrounds can vary greatly.
The interpretations help analyse QTc measurements and assesses cardiac risk.
The algorithm is highly effective in interpreting and alerting on STEMI (ST Segment Elevation Myocardial Infarction).
And how does automatic interpretation work in practice?
See a case study of automatic ECG interpretation with the MESI mTABLET ECG!

Dive into our comprehensive e-book to explore:
- How the ECG works
- How to conduct a resting ECG measurement
- How to interpret the ECG
- Frequently diagnosed conditions
- Automatic interpretation
- A comparison of different resting ECG machines
- Technical specifications of the MESI mTABLET ECG
