Improving efficiency in the Ankle-Brachial Index (ABI) screening test through automated innovative technology

Lower extremity arterial disease (LEAD), a chronic progressive disease, is characterized by multiple risk factors, such as advanced age, ethnicity, genetics, smoking/tobacco consumption, and diseases, such as diabetes, hypertension, dyslipidemia, hyperhomocysteinemia, chronic renal insufficiency, and others.
LEAD is widely prevalent, with around 29% of individuals aged 50 years or older in the US (with tobacco consumption or diabetes history) suffering from the disease [1].
Ankle-Brachial Index (ABI) is a noninvasive vascular screening test, calculated by dividing the highest systolic pressure in the ankle with the highest systolic pressure in the arm [1, 2, 3]. The test is highly sensitive and specific, with very well-established accuracy and is widely used for the initial diagnosis of LEAD.
Traditionally, Ankle-Brachial Index (ABI) measurement has been used as a first-line screening test to detect the lower extremity artery disease, and the Doppler method is designated as the gold standard for the diagnosis. The standard Doppler method requires a Doppler device to detect signals within the arteries, and the sequential systolic blood pressure (SBP) measurement of the four limbs. The method, however, is time consuming and requires trained personnel, which is a major disadvantage. In the search of an easier, faster, and more efficient alternative, clinicians are now utilizing a novel diagnostic technology, based on oscillometry and plethysmography, which employs an automatic blood pressure device, theoretically minimizes observer biases, and does not require any special training [5].
Several studies, including a recent study conducted and published in the European Journal of Vascular & Endovascular Surgery, have established the accuracy and reliability of ABI measurement by the automated device vs the standard Doppler method. The study enrolled 118 patients with suspected LEAD or at-risk patients and conducted Doppler and oscillometric ABI measurements on the patients by two observers to address intra- and interobserver reproducibility. With Dop-ABI as the reference, the study found the sensitivity, specificity, accuracy, positive and negative predictive values of oscillometric ABI to be as high as 89.1%, 94.4%, 94.1%, 91.8%, and 92.4%, respectively. The study further found high concordance and excellent Intra-observer reproducibility, assessed by intraclass correlation coefficient (ICC), between the methods [5].
The study concluded that using an automated device for LEAD screening has excellent diagnostic performance and therefore can be recommended in primary care where fast, efficient and reliable ABImeasurement is required.
Working towards Early Diagnosis of LEAD
Lower extremity arterial disease (LEAD), a chronic, progressive disease, is a manifestation of systemic atherosclerosis, characterized by triggers such as advanced age, ethnicity, genetics, smoking/tobacco consumption, and certain other diseases. LEAD often results in high cardiovascular mortality risks, functional impairment, and lower quality of life in patients. Patients with LEAD have generally a five to six-fold higher cardiovascular risk of mortality as compared to patients with any other atherosclerotic cause [7].
Though the prevalence data for the disease is limited, as per a study in the US, over 29% of individuals aged 50 years or older (with a history of tobacco use or diabetes), have had LEAD. Another recent population-based study in Sweden highlighted the prevalence of LEAD to be around 18% [1].
Early diagnosis of the disease allows effective treatment and proactive lifestyle changes leading to better prognosis, this is why the early patient evaluation should focus on triggers and risk factor screening for asymptomatic patients and patients with atypical symptoms [7].
Around 40% of the LEAD patients are asymptomatic, with no leg symptoms in the presence of an ABI <0.90 or pulse abolition. Another 50% of the patients have atypical symptoms and only around 10% of patients register typical symptoms, such as intermittent claudication. The claudication remains stable in around 70-80% patients, however, in around 10-20% patients it worsens, and in around 1-2% of patients it progresses to acute limb ischemia [7].
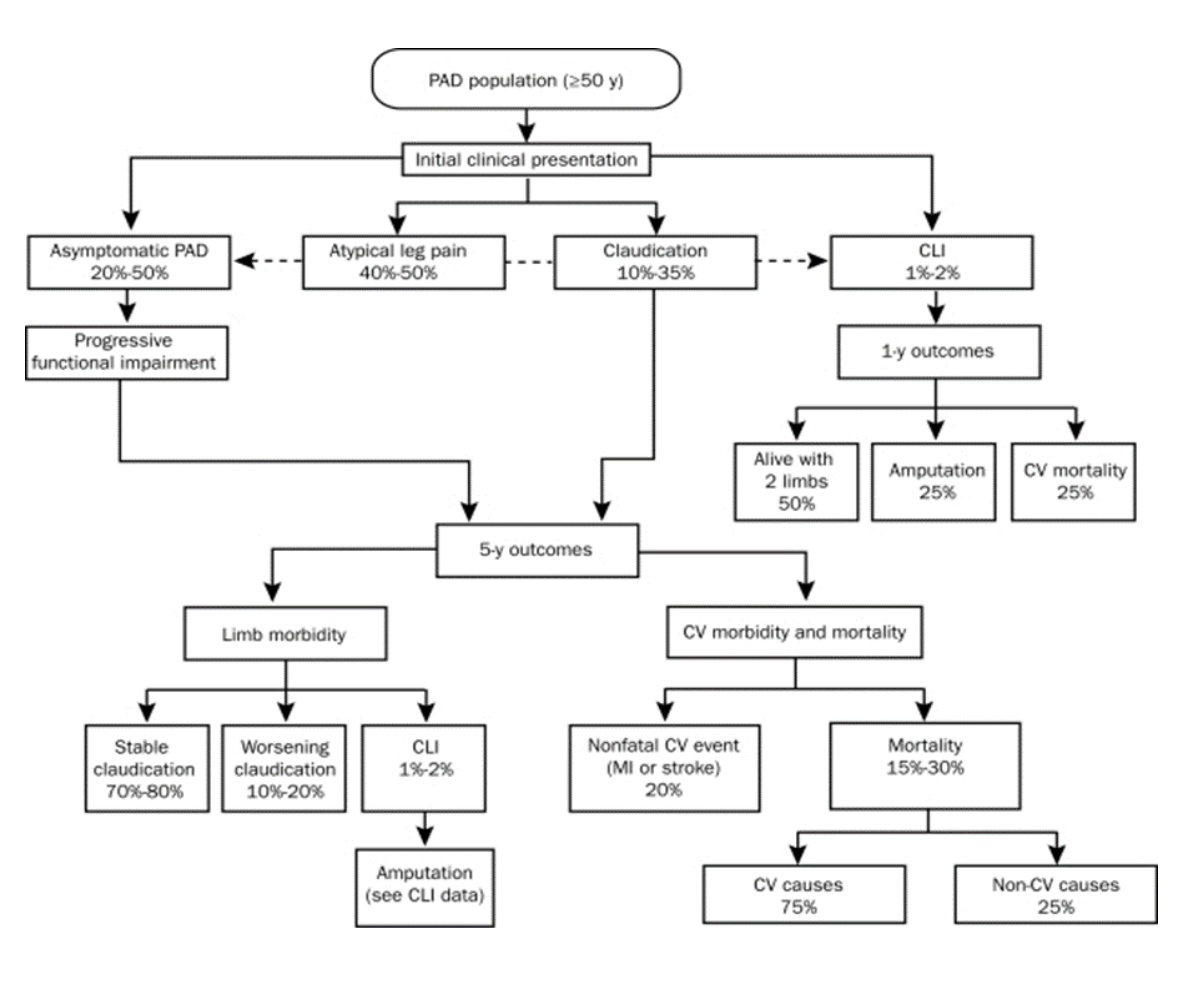
Image Source [8]:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2894725/
What is Ankle-Brachial Index (ABI)?
Ankle-Brachial Index (ABI), is a non-invasive vascular screening test, conducted by the nurses, physicians, surgeons, and podiatrists, to identify the large vessel peripheral arterial disease (PAD). The purpose of the test is to support the diagnosis of vascular disease by using an objective indicator of arterial perfusion to a lower extremity [1, 2].
This test utilizes a device to measure the systolic blood pressure with an inflatable cuff, both at the upper arm and the ankle. The systolic blood pressure measurement equipment can be either manual or digital with automatic electronic readings. The ABI score or the ratio is obtained by dividing the systolic blood pressure recorded at the ankle by the reading at the arm. The ABI ratios of 0.90 to 1.40 fall in the normal range for the adults, and the ratios <0.9 indicate that PAD is present. Further lower readings (< 0.5) suggest that the disease is severe, and the patient might develop ulcers and gangrene in the future [2].
When conducting an ABI measurement, the most widespread method is the Doppler method, where the systolic blood pressures are recorded with a 5- or 10 MHz continuous wave Doppler instrument Traditionally, Ankle-Brachial index (ABI) measurement has been used as a first-line screening test to detect the lower extremity artery disease, and the Doppler method is designated as the gold standard for the diagnosis [1, 3, 5].
Measuring Ankle-Brachial Index (ABI) through automated innovative digital technology
Though the Doppler method is a well-established standard and has high diagnostic accuracy for the Ankle-Brachial index (ABI) measurement, there are some shortcomings associated with the procedure. The procedure is time-consuming, requires trained personnel, which prevents its use in a primary care setting to be widespread. In 2012, the American Heart Association (AHA) highlighted the need for an easier and more efficient alternative method for ABI measurement.
Alternative, automated medical devices are now gaining popularity and attention as the measurement is made much more simple, efficient and requires no special training. Multiple studies have validated the accuracy and sensitivity of the oscillometric method versus the Doppler method, and, based on the advantages automated devices for ABI measurement are already available worldwide [5].
Accuracy and reliability of the Ankle-Brachial Index Measurement using a multi-cuff automated device (MESI mTABLET) vs. the Doppler method [5].
Purpose:
A recent study conducted and published in the European Journal of Vascular & Endovascular Surgery, has established the accuracy and reliability of ABI measurement by an automated device vs the standard Doppler method.
Materials and Methods:
The study enrolled 118 patients with suspected LEAD or at-risk patients, because of the prevalence of two or more cardiovascular risk factors. The men enrolled in the study were all over 60 years of age and women were over 65 years of age.
The researchers conducted Doppler and Automated ABI measurements on the patients by two observers to address intra and interobserver reproducibility. The measurement protocols, laid down by AHA, were followed during the study.
Distribution normality was tested using the Shapiro–Wilk test and the mean ABIs for Doppler & oscillometric methods were compared using Student's paired t-test. The diagnostic capacities assessment including the sensitivity, accuracy, specificity, positive, and negative values for the respective methods to detect a low ABI (≤0.90) was performed using Cohen's kappa coefficient. The intra and interobserver measurement variability was first assessed through the intraclass correlation coefficient (ICC) of the agreement for each method. A second analysis of intra and interobserver reproducibility was conducted using the Bland–Altman method.
Results:
With Dop-ABI as the reference, the study found the sensitivity, specificity, accuracy, positive and negative predictive values of the automated ABI to be as high as 89.1%, 94.4%, 94.1%, 91.8%, and 92.4%, respectively. The accuracy (patients correctly classified by Osc-ABI in comparison to Dop-ABI) was 94.1% for the 1st measurement of observer 1, 92% for observer 2, and 90.3% for 2nd measurement of observer 1. The study further found high concordance (kappa coefficient 0.80–0.88 with two observers) and excellent Intra-observer reproducibility, assessed by intraclass correlation coefficient (ICC of 0.94 with 95% CI 0.91–0.96), between the methods.
The study concluded that such automated devices used for LEAD detection, have excellent diagnostic performance, and can therefore be recommended in primary care where fast, efficient and reliable screening is required.
Emerging Automated Devices
There are various advanced examples of the emerging innovative measurement devices and MESI mTABLET system is one of them. The MESI mTABLET diagnostic system is an all-in-one comprehensive system of top-notch diagnostic modules, patient records, and medical apps [10]. The system includes Automated wireless Ankle-Brachial Index with 3CUFF™ technology, which allows simultaneous measurement of brachial and ankle pressures. It also incorporates PADsense™ algorithm for the detection of severe Peripheral Arterial Disease.
All measurements and patient data are automatically stored and synchronized with the built-in electronic medical record – MESI mRECORDS, available on the MESI mTABLET and from any web-enabled device, simply and securely [11]. This non-invasive device simultaneously measures the Ankle-Brachial Index (ABI) and uses waveform analysis and vascular evaluation technology to generate diagnostic information. The use can be expanded through additional measurement applications, such as pulse wave velocity, averaging blood pressure, etc. The device’s capacity to evaluate patients highly correlates with classic Doppler measurement [12].

The device further has some unique features such as:
Objective results obtained through diagnostic measurements, triage, specialist opinions, consultations, and other data to enable progressive analytics.
Constant upgrades with additional diagnostic tools and medical apps to boost functionality.
Consistent formats to enhance communication reduce reporting inconsistencies and improve diagnosis and treatment time [15].
The take-home messages
LEAD is a highly prevalent disease, with morbidity and mortality similar to coronary artery disease, however, the disease is less accurately investigated and consequently less treated. The existing Doppler method for Ankle-Brachial Index (ABI) measurement, although effective, has limitations of usage in primary care settings leading to lower diagnosis and treatment of the disease.
These limitations of existing methods highlight a latent need for the development of new non-invasive, efficient diagnostic methods. Alternatively, the newly emerging automated plethysmographic technology has demonstrated considerable potential to address the need for simple, cost-effective, accurate, and timely diagnosis of LEAD. With the ongoing disruptive innovations, this type of technology is sure to improve the patient diagnosis and prognosis in the LEAD.
