The 6-Minute Walk Test (6MWT): A clinical overview for healthcare professionals
This blog provides detailed information on a simple but increasingly important test in medical diagnostics: the 6-minute walk test. It discusses when and why we perform it, its contraindications, how it is conducted, the factors affecting its variability, and its clinical implications. You can also watch the content as a video lecture.

In this blog you will learn:
What is the 6MWT?
What is the purpose of the 6-minute walk test (6MWT)?
What are the indications for the 6-minute walk test (6MWT)?
What are the contraindications for the 6-minute walk test (6MWT)?
What do we need for the 6MWT?
How do we perform the 6MWT?
What affects the test’s variability?
What do the results tell us?
What is the test’s prognostic value?
The 6-minute walk test (6MWT) in the management of heart failure patients
The 6-minute walk test (6MWT) in pulmonary arterial hypertension
The 6-minute walk test (6MWT) in assessing respiratory function
The 6-minute walk test (6MWT) on assessing the functional fitness of seniors
What is the 6-minute-walk test (6MWT)
The 6-minute walk test measures the distance that a patient can quickly walk in 6 minutes on a flat surface.
The standardisation by the American Thoracic Society (ATS) made the 6MWT a standardised time test for assessing a patient’s functional capacity. It assesses various organ systems involved in walking and exercise, including the cardiac and pulmonary systems, peripheral and systemic circulation, neuromuscular units, and muscle metabolism.
Here is a video lecture on the various aspects of the 6-minute walk test, its performance and interpretation, delivered by Dr. Anže Žgank:
The 6-minute walk test: why and how?
What is the purpose of the 6-minute walk test (6MWT)?
Aerobic capacity and endurance are useful indicators, e.g. for monitoring progress or determining the general level of preparedness of elite athletes. However, they are also holistic diagnostic indicators of the state of cardiopulmonary and musculoskeletal systems involved in physical exercise, which also makes this kind of testing very useful in diagnosing and monitoring a number of diseases.
In difference to stress ECG, which offers diagnostic information at maximal exercise capacity, the 6MWT assesses functional capacity at submaximal level, at everyday physical activity levels [2]. This means that it can also be used for patients who are not capable of performing other functional capacity tests, e.g. the cardiolpulmonary exercise test (the 6MWT actually correlates well with the VO2 max, measured with this particular test). It is thus a useful evaluation method for a wide variety of conditions. [1]

What are the indications for the 6-minute walk test (6MWT)?
The indications can be divided into three groups: [1]
Pre- and post-treatment testing: The 6MWT is used to assess the success of various treatments. In other words, to monitor progress of the functional capacity of the patient after procedures like lung transplant, lung resection, lung volume reduction surgery, pulmonary rehabilitation, and treatment for conditions like pulmonary hypertension, COPD and heart failure. In these cases, several tests will be performed at certain intervals within a specific period of time.
One-time measurement: In this group of conditions, the 6MWT is used as a one-time measurement to assess the functional status of patients with conditions like cystic fibrosis, COPD, peripheral vascular disease, fibromyalgia, heart failure and geriatric patients.
Morbidity and mortality prediction: The 6MWT is used to predict morbidity and mortality in patients with COPD, heart failure and pulmonary hypertension.
Clinicians also use the 6MWT for a wide variety of non-cardiopulmonary diseases, including neuromuscular conditions such as Charcot-Marie-Tooth disease (i.e. inherited neurological disorders that mainly affect the peripheral nerves) and myasthenia gravis (i.e. chronic autoimmune neuromuscular disorder that primarily affects the muscles responsible for voluntary movements) [3, 4].
What are the contraindications for the 6-minute walk test (6MWT)?
The 6MWT has absolute and relative contraindications:
Among others, absolute contraindications include:
unstable angina,
myocardial infarction in the last month,
syncope,
symptomatic severe aortic stenosis,
acute pulmonary embolus or pulmonary infarction.
Among others, relative contraindications include:
a resting heart rate over 120 BPM,
a systolic blood pressure over 180 mm Hg,
a diastolic blood pressure over 100 mm Hg,
cardiac conditions like high-degree atrioventricular block, hypertrophic cardiomyopathy and left main coronary stenosis or its equivalent,
significant pulmonary hypertension.
What do we need for the 6MWT?
The environment
The 6MWT is best conducted indoors; performing it outdoors may affect the test result. We need a flat and enclosed corridor with a durable surface, at least 30 m long. It is important to choose a location that is not very busy (as other people can inadvertently interfere or distract the patient), but where a fast emergency response can be initiated. [1]
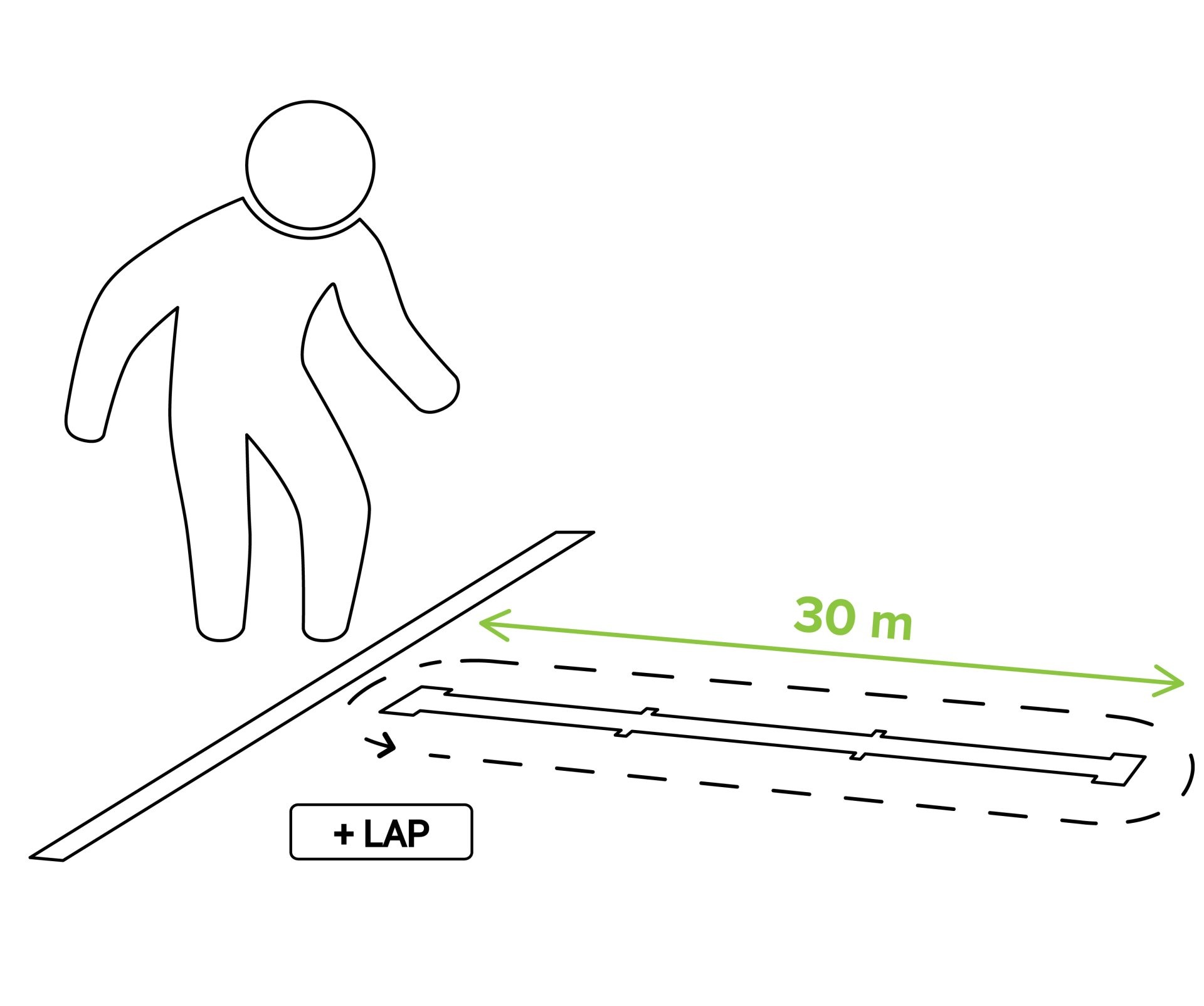
The track
The walking course should measure 30 m in length. Going up and down the corridor once is regarded as one lap (60 m). The corridor should have clear markings every 3 m. At both ends of the course, there should be designated turnaround points, typically indicated by the placement of cones, such as bright orange traffic cones. Additionally, the starting line, which signifies the beginning and end of each lap, should be clearly demarcated on the floor using brightly-coloured tape. [5] [6]
The equipment of the examiner
The examiner needs: [1]
A stopwatch
Two small cones to mark the turnaround points
Tape for the 3 m marks and the starting line
A chair (for the patient to sit on before and after the test)
A source of oxygen
Blood pressure meter and oximeter
Telephone (for emergencies)
Automated electronic defibrillator (for emergencies)
The equipment and preparation of the patient
Patients should be dressed comfortably in appropriate clothing and wear suitable walking shoes. They should also be asked to utilise any regular walking aids; please document them on the assessment form. [5] [6]
Prior to initiating the 6MWT, patients should rest for a minimum of 10-15 minutes.
Patients on long-term oxygen therapy should continue with their usual oxygen flow rate, following the direction of their physician or a predefined protocol.
Patients should also be reminded to adhere to their regular medication regimen. Please note the medication type, dosage, and the time elapsed since the last dose before the test.
The patient does not need a warm-up before the test.
Any future test repetitions should be performed at the same time of day.
How do we perform the 6MWT?
The test is performed in 10 steps.
Have the patient seated in a chair near the starting point, with a minimum 10-minute rest. Assess for contraindications, measure blood pressure and pulse, and check if the patient has appropriate clothes and shoes.
Perform pulse oximetry.
Document the baseline heart rate and oxygen saturation (SpO2).
Have the patient stand and assess baseline dyspnea and overall fatigue using the Borg scale.
Prepare to initiate the test by setting a timer for 6 minutes and positioning yourself at the starting point.
Briefly explain the test to the patient: “The objective of this assessment is to cover as much distance as possible in 6 minutes.” Demonstrate one lap for a visual example.
When the patient starts walking, start the timer. Do not accompany the patient during the test. Monitor the SpO2 rate throughout.
Keep a record of the number of laps completed and provide encouragement as needed. Standardised phrases are used to inform the patient of the remaining time and to provide mild encouragement. If the patient needs a rest during the test, they should receive it as needed by leaning on a wall, but the timer should not be stopped.
After the test, reassess the vital parameters, dyspnea, and fatigue using the Borg scale. Ask about any reasons that may have prevented the patient from walking further.
Calculate the total distance walked, rounding the measurement to the metre.
The reasons for stopping a 6MWT immediately include intolerable dyspnea, chest pain, leg cramps, diaphoresis, staggering, and pale or ashen appearance. [5] [6]
What affects the test’s variability?
Several factors can influence the variability of 6MWT results. These include: [1]
Patient characteristics: Factors such as age, sex, height, weight, and cognitive status play a role.
Underlying diseases: Preexisting medical conditions can impact test outcomes.
Corridor length: A shorter corridor yields shorter distances covered during the test.
Supplemental oxygen: Patients using it may achieve greater distances.
Experience with previous tests: If the patient has performed the test before, the total distance covered may increase.
What do the results tell us?
The result can be given as the absolute distance covered during the test, or the difference between the distances of two consecutive tests can be noted.
Please note that the 6-minute walk distance (6MWD) alone is not a specific diagnostic measurement. The following factors should be considered for clinical significance of the result.
Underlying diseases
While the 6MWT provides valuable information, the test alone cannot diagnose specific conditions. Many underlying diseases can affect the distance. The clinical significance of the result depends on the patient’s condition, which may have already been diagnosed or is still unknown. Therefore, it’s crucial to interpret the results alongside those of other diagnostic procedures.
SpO2 monitoring
Maintaining stable SpO2 levels is important during the 6MWT. A drop in SpO2 by more than 5% may indicate an underlying respiratory or cardiac disorder.
What is the test’s prognostic value?
The 6MWT is not only diagnostic but also holds significant prognostic value. Studies have shown its relationship with morbidity and mortality in various patient populations: [1]
COPD patients: An Indian study showed that the 6MWT distance is a superior predictor of mortality compared to measures like FEV1, FVC, and the Tiffeneau index. [7]
A Canadian study on COPD patients found a survival correlation between COPD and 6MWD: the patients who could walk over 250 m had a mean survival of about 42 months, while those who walked less than 150 m had a mean survival of 28 months. [8]
Pulmonary fibrosis: Research on patients with pulmonary fibrosis revealed that a decline of 50+ m in a 24-week period was associated with a fourfold increase in the risk of death at one year. [9]
Another study on patients with this disease showed that walking less than 300 m was associated with a 2.4 times higher mortality risk. Similarly, an SpO2 fall of more than 10% increased the mortality risk by 2.9 times. [10]
Pulmonary hypertension: In patients with pulmonary hypertension, a normal 6MWT distance of approximately 500 m indicated an excellent prognosis. Conversely, those who could walk less than 300 m had a poor prognosis. [11]
A systematic review of studies on patients with a pathology found that fall in the 6MWT distance by 14 to 30 m was considered clinically important deterioration. [12]
COVID-19:
The 6MWT has proven its utility during the COVID-19 pandemic. A Danish study highlighted its importance in diagnosing exercise-induced hypoxia in patients just before hospital discharge. This diagnosis holds several key advantages: [13]
Uncovering Underlying Diseases: Patients with exercise-induced hypoxia may have undiagnosed pulmonary or cardiac conditions.
Detecting Complications: COVID-19 is associated with various thromboembolic events, including pulmonary embolism, which can manifest through exercise-induced hypoxia.
Oxygen Therapy Candidates: Identifying patients with hypoxia during exercise is crucial, as they are prime candidates for supplemental oxygen to enhance their functional capacity during rehabilitation after COVID-19. [13]
An Italian study demonstrated the 6MWT’s usefulness in monitoring rehabilitation progress in patients who have undergone intensive care unit (ICU) treatment. This application of the test plays a vital role in ensuring the well-being and progress of patients after their critical care journey. [14]
In an Indian study, patients with pulmonary diseases performed the 6MWT with and without face masks. The results revealed that wearing a mask during the test led to shorter walking distances. This factor has become particularly relevant during the COVID-19 pandemic, underscoring the importance of considering external variables when assessing 6MWT results. [15]
The 6-minute walk test (6MWT) in the management of heart failure patients
Given the significant impact of heart failure on functional exercise capacity, particularly in individuals with class C and D disease, the 6-Minute Walk Test (6MWT) emerges as an exceptionally suitable assessment method. It offers affordability, demands no specialised equipment, maintains non-invasiveness, and is generally well-tolerated by most patients, except for those with strong mobility limitations.
A decline in 6MWT performance among heart failure patients correlates with heightened risks of mortality, non-fatal cardiovascular events and hospitalisations, particularly within the B and C subclasses of heart failure.
To read an extensive article on the risk factors and prevalence of heart failure, its morbidity, mortality, economic impact and the use of the 6MWT in patients with this condition, click here.
The 6-minute walk test (6MWT) in pulmonary arterial hypertension
The 6MWT serves as a valuable prognostic indicator for long-term PH-related mortality and the risk of hospitalization. In fact, it has been discovered that patients capable of walking at least 400 m within the allocated 6-minute timeframe generally exhibited the most favorable prognosis. The 6MWT is also used for following the progression of the disease and assessing functional capacity.
To find out more about pulmonary hypertension, its burden and morbidity, and the way the 6MWT is used in assessing patients with this disease, click here.
The 6-minute walk test (6MWT) in assessing respiratory function
In the context of pulmonary conditions, healthcare professionals commonly recommend the 6-Minute Walk Test (6MWT) for specific patient groups. This includes individuals awaiting lung transplantation and those diagnosed with cystic fibrosis. The 6MWT also proves valuable in assessing post-surgical mortality among patients who have undergone lung resection and in determining the severity of pulmonary arterial hypertension, a complex cardiopulmonary condition that presents significant treatment challenges.
To find out more about the use of the 6MWT in pulmonary issues and specifically how it is used in patients with COPD and COVID 19, click here.
The 6-minute walk test (6MWT) on assessing the functional fitness of seniors
Assessing the exercise capacity of seniors, a diverse demographic united only by their age, serves the crucial purpose of identifying those who require tailored exercise instructions and recognising individuals who may be unable to engage in physical activity promptly. This underscores the vital utility of the 6MWT, which provides a comprehensive evaluation of cardiopulmonary and muscular fitness.
To find out about the average walking distances of healthy seniors and the effect of various conditions on their results, click here.

Dr. Anže Žgank, pulmonology resident at University Medical Centre Ljubljana, Slovenia
Dr. Anže Žgank graduated from the Faculty of Medicine at the University of Ljubljana (Slovenia) in 2018. He then began his internship at General Hospital Celje, where he also started his residency in internal medicine in 2019. Since 2020, he has been employed as a resident in pulmonology at the Clinical Department of Lung Diseases and Allergy at the University Medical Centre Ljubljana.
