What you need to know about the latest Peripheral Arterial Disease guidelines
Peripheral Arterial Disease (PAD) is a frequent but underdiagnosed condition, often with severe consequences. They can include death, stroke, coronary heart disease, amputations, dementia and cognitive impairment [1]. A late diagnosis therefore represents a significant burden for healthcare, both in terms of finance and manpower. Here are the latest Peripheral Arterial Disease guidelines in a nutshell.

In this blog you will learn:
Peripheral Arterial Disease (PAD), an underdiagnosed condition
Guidelines for Peripheral Arterial Disease (PAD) detection
The price of underdiagnosed Peripheral Arterial Disesase (PAD)
Technological solutions for effective Peripheral Arterial Disease (PAD) detection
Peripheral Arterial Disease (PAD), an underdiagnosed condition
Compared to myocardial infarction and stroke, PAD is underrecognised and understudied. This is also due to its frequently asymptomatic nature:
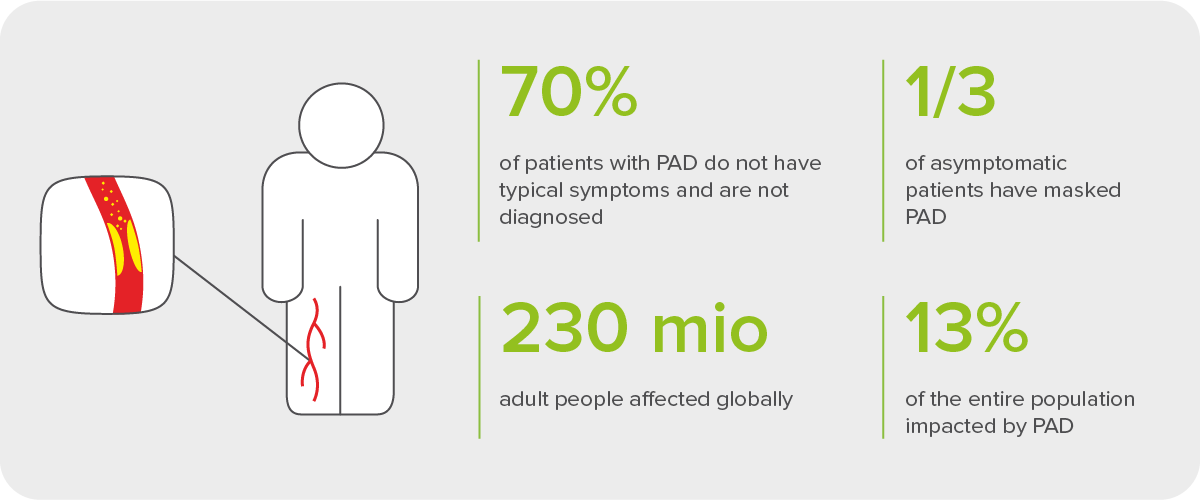
Global Peripheral Arterial Disease (PAD) statistics.
Many patients do not have symptoms of intermittent claudication (leg pain due to obstructed blood flow) or are not mobile enough for the symptoms to show [2]. Sometimes, difficulty walking is attributed to normal ageing or conditions like arthritis [1]. However, according to the REACH (Reduction of Atherothrombosis for Continued Health) registry, PAD patients have a 1 in 5 chance of having a cardiovascular event in 1 year (compared to 1 in 6 for coronary patients and 1 in 7 for patients with a history of stroke) [3].
Systematic ABI check-ups are recommended for all risk groups. TBI or simultaneous ABI-TBI measurement should be used if suspecting medial artery calcification, e.g. in cases of CKD or diabetes.
Guidelines for Peripheral Arterial Disease (PAD) detection
There are four major recent guidelines published in the PAD field, namely:
the 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS) (short: ESC/ESVS Guidelines), and
the Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC-II).
They differ in their focus and partly in their terminology.
The 2024 ESVS Guidelines use the term ‘PAD’ for lower extremity Peripheral Arterial Disease. They focus on its asymptomatic and intermittent claudication phenotypes, with emphasis on early detection methods and collaboration with the patient when determining the treatment.
The American Heart Association Scientific Statement (2021) uses the term PAD as an abbreviation for lower extremity peripheral artery disease – the most frequent PAD occurrence. In has a strong focus on the awareness raising and management gaps in connection with this condition. Consequently, the latest epidemiology and diagnostics are presented in great detail.
The ESC/ESVS Guidelines concentrate on all forms of PAD (i.e. all arterial diseases except those affecting coronary arteries and the aorta). These include LEAD (lower extremity artery disease) and many others. For this reason, the term PAD is often used in plural form. The focus in the Guidelines is on the medical definition of the various PADs and classed recommendations of their treatments.
TASC-II is a successor of the Trans-Atlantic Inter-Society Consensus Document of Management of Peripheral Arterial Disease (TASC, 2000). Similarly to AHA, it aims to raise awareness not only among vascular specialists, but also physicians at primary care level. Like the ESC Guidelines, however, it presents a grading of the recommendations for PAD treatment. The focus of the document is “PAD of the leg” [5].
ESVS Guidelines (2024)
The focus of the European Society for Vascular Surgery (ESVS) 2024 Clinical Practice Guidelines on the Management of Asymptomatic Lower Limb Peripheral Arterial Disease and Intermittent Claudication is on asymptomatic PAD and intermittent claudication. They recommend that focus screening with Ankle-Brachial Index (ABI) measurements should be considered for the following clinically asymptomatic individuals at increased PAD risk: [6]
all individuals aged 65 years or older
all individuals between 50 and 64 years with any of the following risk factors for atherosclerosis:
diabetes
history of smoking
hyperlipidaemia
hypertension
chronic kidney disease
family history of PAD
all individuals younger than 50 years with:
diabetes + one other risk factor for atherosclerosis
all individuals with known atherosclerotic disease in another vascular bed.
Other important focuses are on TBI and the 6-minute test as additional methods in PAD detection, exercise therapy for patients with intermittent claudication, and active participation of the patient in treatment decision. For this reason, the 2024 ESC Guidelines also include a patient-friendly summary of the most important PAD information. You can find out more in this detailed report.
AHA Scientific Statement (2021)
The 2021 AHA Scientific Statement urges that PAD screening with ABI is widely implemented in the following populations:
adults aged 65 or older
people with conventional risk factors:
diabetes
smoking
dyslipidemia
hypertension
It also highlights the following non-conventional risk factors:
hemostatic factors (e.g. fibrinogen): strong predictors for PAD development
some studies state HIV as a risk factor: a sustained CD4 cell count <200 cells/mm3
lead exposure (traditionally underrated in connection with CVD in general): blood lead levels were found to be 14% higher in patients with PAD than those without
cadmium: cadmium levels increase with PAD severity
air pollution (living in urban areas: 2-3 times higher PAD risk; living near major roadways: ABI decrease)
depression: either due to medication non-compliance or low physical activity
sedentary lifestyle: a factor affecting (at the very least) symptomatic PAD in terms of worse biomarkers.
You can find more information about the American Heart Association and its Scientific Statement in this detailed report. An important distinction is that the Statement also highlights sedentary lifestyle, environmental factors (air pollution) and depression as contributing factors to PAD, in contrast to the other two less recent guidelines.
ESC/ESVS Guidelines (2017)
The ESC/ESVS Guidelines underline an interdisciplinary approach to PAD, calling for a so-called “vascular team”. A detailed clinical history (CV risk factors, comorbidities, symptoms in various vascular territories) and physical examination of the patient are vital. The same goes for the lifestyle, dietary and physical activity assessment. It is recommended that detailed questionnaires be used in the process.
In this, the ABI is denoted as a useful non-invasive tool for diagnosing and monitoring LEAD as well as a strong marker of general CV and atherosclerosis risk.
ESC guidelines recommend early ABI measurement for:
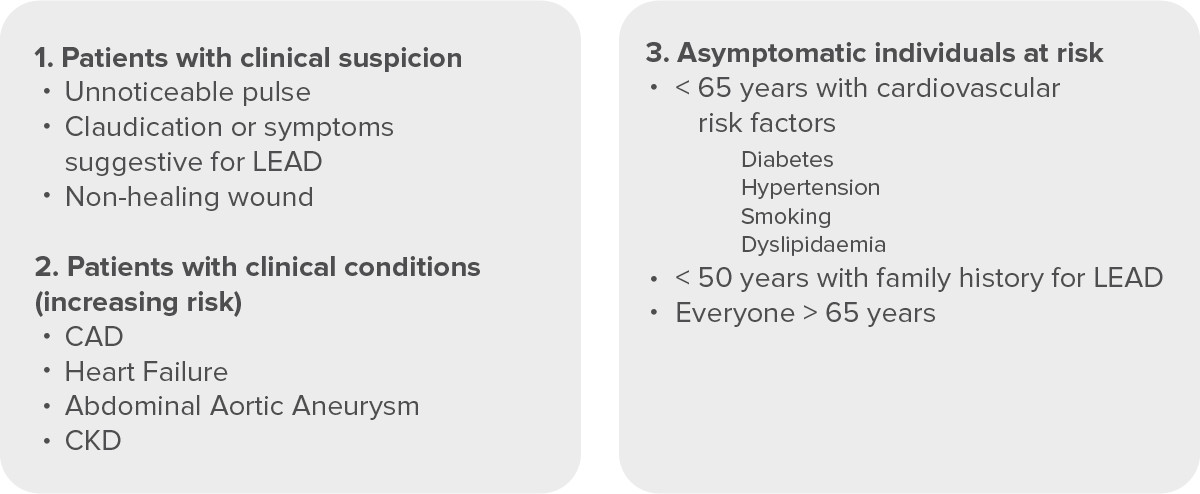
Peripheral Arterial Disease (PAD) risk groups according to ESC guidelines.
TASC-II (2007)
In addition to the risk factors for PAD, TASC-II focuses on the consequences of PAD, among others:
a five-year prognosis for a person with intermittent claudication,
effect of risk factors on developing CLI (ABI values, diabetics, smokers, age over 65, lipid abnormalities),
one-year prognosis for CLI patients,
two-year prognosis for below-knee amputees.
In this, the risk of CV events in PAD cases is connected with the severity of PAD, which is defined by the ABI measurement.
TASC-II notes that early identification of PAD with patients who are at risk of developing foot problems is essential for amputation prevention. [5] This is well in line with the ESC Guidelines, which were issued a decade later, stating that ABI can help identify one’s risk for lower-extremities events to prevent foot wounds. [1]
In the case of chronic wounds, determining the correct therapy is essential as the consequences of applying compression in the case of incompressible arteries can be extremely severe. The WOCN (Wound, Ostomy and Continence Nurses Society) guidelines [4] state that an ABI measurement should be performed before prescribing compression therapy for venous insufficiency, thrombotic risk or lower limb ulcers. TASC-II provides the following reference values for ABI measurement [5]. They are presented below in combination with the WOCN guidelines for medical compression:
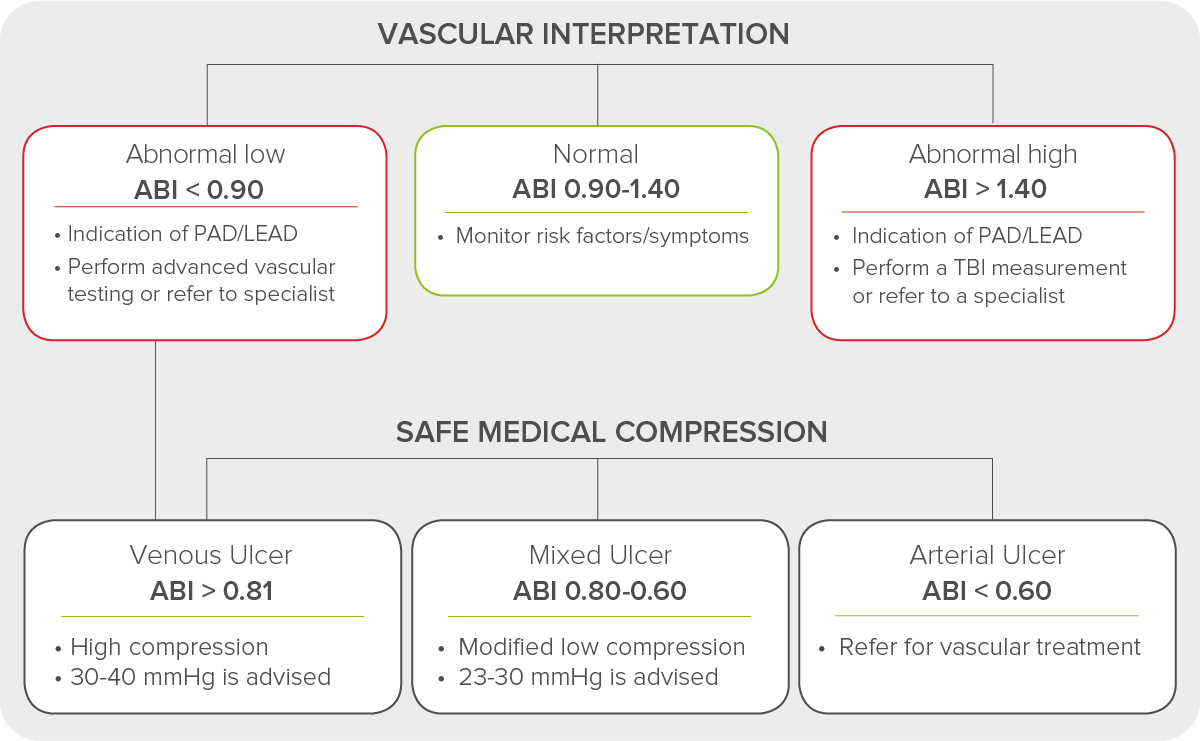
ABI reference values from TASC-II in combination with WOCN guidelines for safe medical compression.
The price of underdiagnosed Peripheral Arterial Disease (PAD)
An important takeaway from these three latest Peripheral Arterial Disease guidelines is that PAD is a complex disease reflecting many factors such as genetics, contemporary lifestyle (sedentary behaviour), the quality of the environment, physical activity as well as mental aspects of our being, such as depression [1]. Each new set of guidelines reveals more on this complex yet growing phenomenon, and an additional price that we will have to pay if it continues to be underdiagnosed.
The evidence from the latest Peripheral Arterial Disease guidelines shows that PAD is a strong predictor of stroke and myocardial infarction, and thus strongly associated with mortality. It is also associated with serious complications, such as amputation and acute limb ischemia, which profoundly affect one’s quality of life [1]. Therefore, a delayed diagnosis represents a considerable burden for the patient and healthcare. Screening for PAD with ABI, especially in high-risk groups, is connected with significant cost reduction and gain in quality-adjusted life-years.
Technological solutions for effective Peripheral Arterial Disease (PAD) detection
ABI measurements with standard devices like the handheld Doppler probe are time-consuming and require trained specialised staff. This makes ABI measurements with traditional methods diffcult to access, and can result in many patients with PAD going undetected and untreated.
Digital solutions successfully fill this gap, and make check-ups more efficient and convenient.
With modern equipment such as the MESI mTABLET ABI, the ABI measurement only takes one minute. It can become easily available in primary care and areas like woundcare, where it helps distinguish between venous and arterial wounds, determine appropriate compression therapy, and discover PAD in high-risk patients, including diabetics.
Why choose the MESI mTABLET ABI?
1-minute, easy and reliable measurement with pulse waveform interpretation
3CUFF™ technology permits simultaneous measurement
PADsense™ algorithm for detection of severe Peripheral Arterial Disease
Multiple cuff sizes available
