Frequently diagnosed conditions with spirometry

NORMAL LUNG FUNCTION
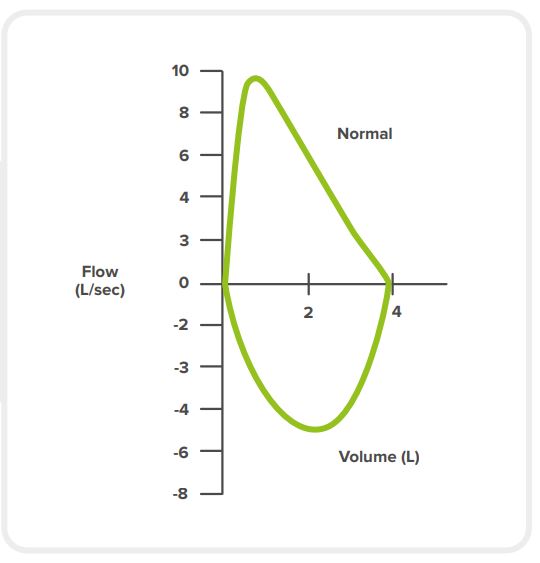
A normal lung function flow-volume graph has the following characteristics:
a fast rise to the highest flow rate
a nearly linear fall in the flow
OBSTRUCTIVE CONDITIONS
Obstructive conditions are marked by reduced airflow (how fast you can inspire and expire). [11] [21]
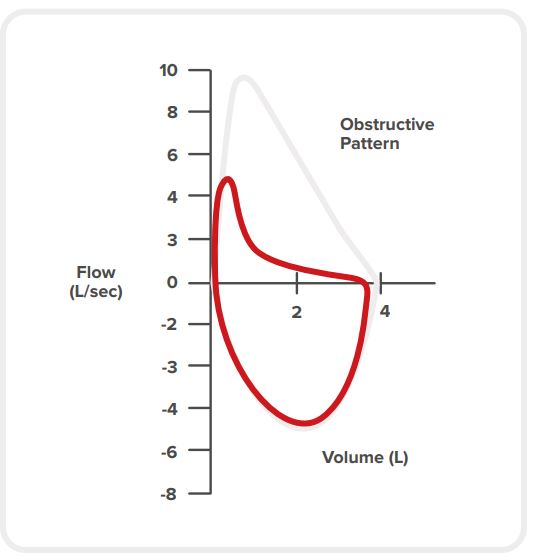
Obstruction is characterised by: [11] [22] [4]
normal or reduced VC
normal or reduced FVC
strongly reduced FEV1 (due to airway resistance when breathing out)
strongly reduced FEV1/FVC ratio
concave flow–volume loop
abnormally enlarged lungs (hyperinflation)
Asthma
Asthma causes various degrees of breathing problems due to inflammation and muscle tightening around the airways, which limits the airflow. It is one of the most common chronic, non-contagious lung diseases in people of all ages. [4] [7] [23]
SYMPTOMS
The most common symptoms of asthma are:
wheezing (a whistling sound during breathing),
breathlessness (dyspnea),
chest tightness (it can feel as if one had a tight band tied around it),
coughing.
Asthma can sometimes get worse for a period of time (from a few minutes to days). This is called an asthma attack. In addition to persistent wheezing and coughing, asthma attacks can cause:
onstant breathlessness (which affects eating and sleeping),
fast breathing,
fast heart rate,
exhaustion,
dizziness,
blue lips or fingers,
fainting.
CAUSES
Asthma often starts in childhood, when the immune system is still developing. It can result from many risk factors (allergens in the environment, viral infection, family history, race or ethnicity, sex). The risk factors can combine.
Asthma can also appear later in life, e.g. due to obesity or occupational hazards (exposure to industrial dusts or chemicals).
Asthma attacks are caused by triggers:
environmental factors (allergens),
extreme heat or cold,
stress,
physical exercise,
or any combination of them.
DIAGNOSTIC METHODS
The main tests used to help diagnose asthma are:
Allergy tests
Imaging test (chest X-ray)
Spirometry:
Peak flow test: The test measures how quicky a patient can expire. It can be done with the peak flow meter or a spirometer. The score can indicate if the airways are narrowed. [27]
Methacholine challenge test (bronchoprovocation test) or hystamine challenge test: Asthma is characterised by hyperresponsiveness of the airways to certain substances such as allergens. In this test, the patient’s baseline lung function (FEV1) is first established with spirometry. Then, the patient inhales certain allergen substances (‘provocation’). Asthma can be indicated by a significant fall in FEV1.
Asthma according to ERS guidelines
The ERS guidelines [28] define asthma as a combination of typical symptoms (breathlessness, cough, wheezing, chest tightness) and objective demonstration of excessive airway calibre fluctuation with at least one of the following results:
1. Peak flow variability ≥20% or spontaneous variation in FEV1 ≥12% and 200 ml
2. Reversibility after bronchodilator inhalation with improvement in FEV1 of ≥12% and 200 ml
3. Airway hyperresponsiveness: PC20-M (or H) <8 mg/ml (or 16 mg/ml in patients treated with inhaled corticosteroid), PD mannitol < 625 mg or FEV1 fall ≥10% after exercise
PC20-H: provocation concentration causing 20% fall in FEV1 with histamine
PC20-M: provocation concentration causing 20% fall in FEV1 with methacholine
PD: provocation dose
4. Improvement in FEV1 ≥12% and 200 ml after a 2-week course of oral corticosteroid or a 4-6-week
course of inhaled corticosteroid
TREATMENT
There is no cure for asthma so far, but treatment can help with symptom control. The patient usually creates an individual treatment plan with their doctor or asthma nurse.
The main asthma treatment method is inhalers. Preventer inhalers are devices used to reduce the inflammation and sensitivity of the airways; they need to be used daily, even if the symptoms are not present. Most asthmatics also receive reliever inhalers for treating the symptoms when they occur. In severe cases, tablets and other treatments may be needed. [29] [67]
COPD
Chronic obstructive pulmonary disease (COPD) is an incurable, progressive chronic lung disease. It is the third leading cause of death worldwide. [30]
COPD can result in a number of complications, including: [31]
Respiratory infections due to weakened respiratory immunity. Patients with COPD are more susceptible to colds, pneumonia and the flu. This worsens the breathing difficulties and can damage the lung tissue even more.
Heart conditions. COPD can increase cardiovascular risk, including that of heart attack.
The risk of developing lung cancer increases.
Pulmonary hypertension: high blood pressure in the arteries bringing blood to the lungs.
COPD is difficult to cope with and prevents many activities due to breathing difficulties. This can contribute to the onset of depression.
SYMPTOMS
The patient experiences growing respiratory problems and airflow limitation. In numerous patients, chronic cough (with or without sputum production) can appear years before the airflow gets limited. Other symptoms include chest tightness, fatigue, and chronic and progressive shortness of breath (dyspnea). [31] [32]
Differential diagnoses should be considered. For example, shortness of breath and cough are also symptoms of COVID-19, pneumonia or asthma.
CAUSES
The key preventable risk factor is smoking. Other causes include environmental or occupational exposure to irritants, extreme heat or cold as well as genetic conditions: protein alpha 1-antitrypsin (AAT) deficiency affects the body’s ability to produce this protein, which protects the lungs. [31]
Triggers for COPD exacerbations: viral or bacterial infections in half of the cases, and environmental factors in the other half.
DIAGNOSTIC METHODS
COPD is diagnosed on the basis of:
medical history (development of patient’s symptoms, risk factors, family history)
questionnaires [35]: The Modified British Medical Research Council (mMRC) Questionnaire assesses breathlessness – from grade 0 (breathlessness with strenuous exercise only) to grade 4 (affecting daily activities, including the ability to go out of the house). COPD Assessment Test (CAT) assesses the effect of COPD on the patient’s daily functioning, with scores from 0 to 40.
spirometry (FEV1/FVC): Spirometry is used for measuring the airflow limitation. It is essential in discovering COPD at its early stage, i.e. before obvious symptoms appear. In this, bronchodilators (medications used to relax bronchial muscles) are used, so the air can pass through the lungs more easily. [33]
An official diagnosis of COPD is made on the basis of post-bronchodilator FEV1/FVC <0.70; this shows persistent airflow limitation. [30]
COPD according to GOLD
Post-bronchodilator FEV1/FVC shows the severity of airflow limitation. On its basis, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines classify patients into four categories [34]:
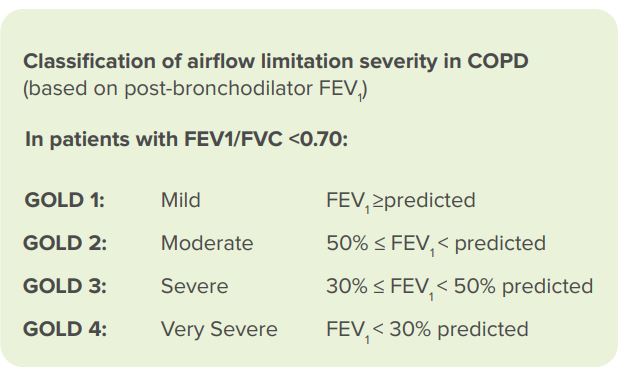
FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity.
TREATMENT
There is no cure for COPD as yet. When managing COPD, different therapies are used to reduce the symptoms and their severity, enhance life quality, and increase exercise tolerance. Smoking cessation and avoiding harmful environmental exposures are crucial.
Treatments include:
Inhalers:
Bronchodilator inhalers relax and widen the airways. They include beta-2 agonists (for opening bronchial tubes) and antimuscarinics (for relaxing the airways by blocking the nerve impulses that cause the airway muscles to contract). [36] Bronchodilator inhalers may be short-acting (only used when experiencing breathlessness) or long-acting (used with regular symptoms or exacerbations).
In serious cases, steroid inhalers are used; they contain corticosteroid, which reduces the inflammation (swelling) of the airways. [37]
Tablets (bronchodilator; mucolytics – against phlegm; steroids; antibiotics)
Pulmonary rehabilitation (a combination of education and exercise)
Oxygen therapy
Surgery:
bullectomy: removal of air pocket in the lungs
lung volume reduction surgery: removing a damaged lung section so the other parts can function better
lung transplant
COPD is a mixture of a number of conditions; chronic bronchitis and emphysema are the most prominent. They have similar symptoms but affect different parts of the lungs. Chronic bronchitis affects the airways (the tubes that enable air to go in and out of the lungs) while emphysema affects the alveoli (the air sacs at the end of the airways), causing their walls to rupture. This creates larger air spaces, reducing the amount of oxygen that reaches the bloodstream. [7] [38] [39]
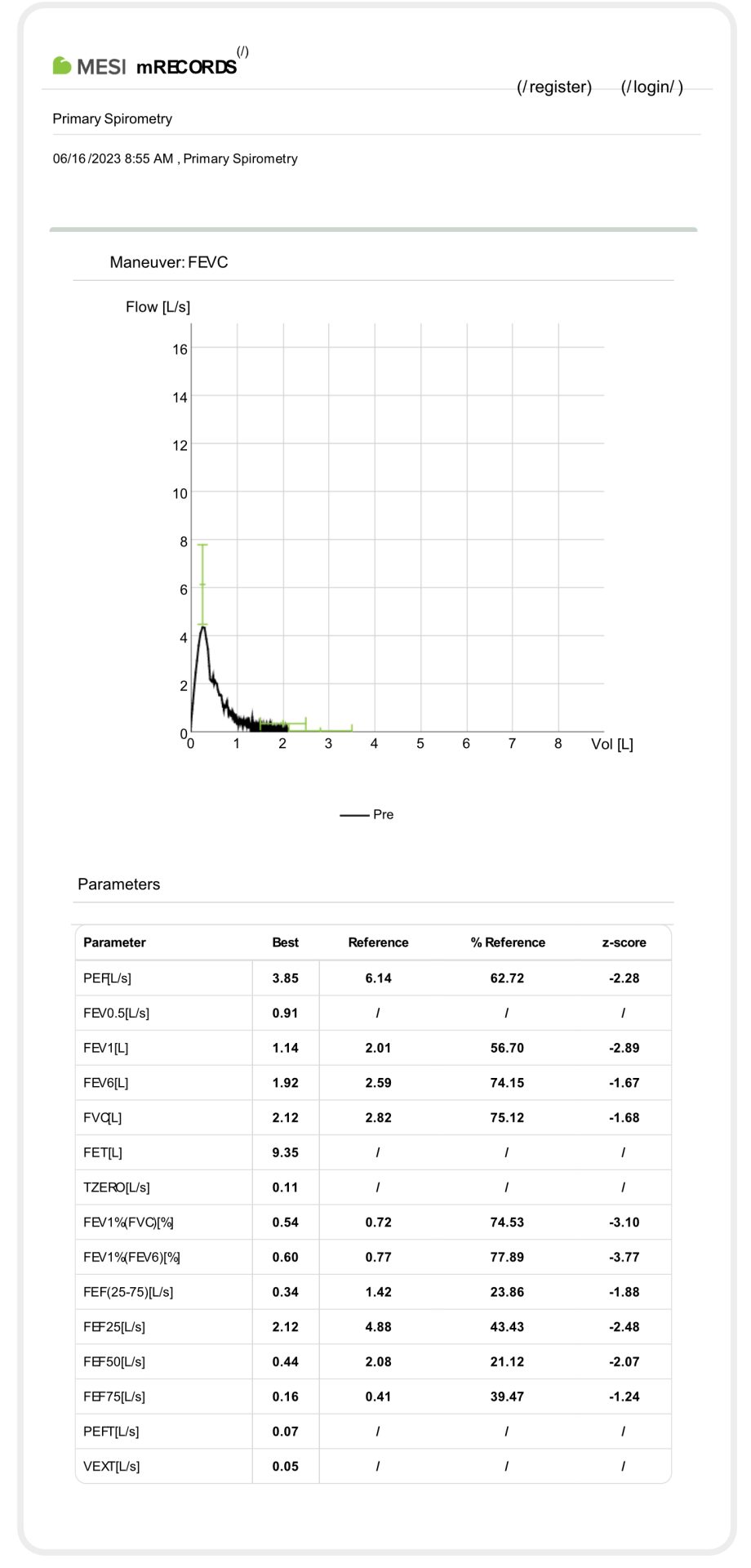
Example of spirometry measurement in a long-year chronic smoker with COPD suspicion:
BRONCHITIS
Bronchitis is the inflammation of the bronchial tubes. This results in coughing bouts with mucus, chest pain, wheezing and shortness of breath. There are two main bronchitis types, acute and chronic. [38]
Chronic bronchitis is a type of COPD and develops gradually; the symptoms may fluctuate, but never completely disappear. Long-term bronchial inflammation causes mucus build-ups in the airways, which blocks the narrowed tubes even more. The patient develops a chronic cough due to constantly trying to clear their airways, and may also experience frequent bacterial or viral infections. [33]
Acute bronchitis usually results from infections and disappears in one or two weeks. The cough is worse at night or during physical exertion.
CAUSES
Acute bronchitis is usually caused by respiratory infections due to bacteria and viruses: rhinovirus (common cold), flu, respiratory syncytial virus (RSV), COVID-19, etc. It is not contagious, but the viruses and bacteria that cause it are. [40]
Chronic bronchitis is not contagious. It is connected with a number of risk factors:
smoking (active or passive)
older age
environmental or occupational exposure to harmful fumes and dust types
a family history of COPD
a history of respiratory disorders (cystic fibrosis, asthma, bronchiectasis)
gastroesophagal reflux disease (GERD)
DIAGNOSTIC METHODS
With acute bronchitis, the diagnosis is primarily clinical (relying on physical examination and medical history rather than laboratory tests or imaging). [41]
Chronic bronchitis is diagnosed by means of:
spirometry
chest X-ray (to check for heart failure and other conditions that contribute to breathing difficulties)
computed tomography (CT): for a detailed lung examination, especially when suspecting COPD (emphysema)
Patients with chronic bronchitis must be tested for COPD.
TREATMENT
Patients with acute bronchitis are usually not medicated. In case of viral infections, antivirals may be prescribed. The same goes for antibiotics in bacterial infections, especially to patients with other lung diseases or progression to pneumonia. [42] [43]
Chronic bronchitis is not curable. Stopping the exposure to irritants will cause it to subside.
Treatments for chronic bronchitis include:
bronchodilators,
oxygen therapy and
steroids. [33]
EMPHYSEMA
Emphysema is an incurable progressive lung disease. It affects the alveoli – the place where the blood and the lungs exchange oxygen and carbon dioxide in the breathing process. [44]
CAUSES
The primary cause is long-term exposure to cigarette smoke. This is followed by environmental pollutants (e.g. air pollution, industrial chemicals). Genetic deficiency of the alpha-1 antitrypsin (AAT – a protein that helps protect the lungs against inflammation and infection), can make the patient more susceptible toenvironmental factors; this increases the risk of emphysema and COPD.
SYMPTOMS
Shortness of breath: The main symptom. Initially with exertion only, but it may result in difficulty breathing at rest as the disease progresses.
Coughing: Many patients with emphysema also have chronic bronchitis and therefore chronic cough. [45]
Wheezing
Barrel chest: It may develop due to increased lung volume and overinflation of the lungs.
Weight loss: Due to breathing effort and reduced appetite in advanced stages.
DIAGNOSTIC METHODS
Physical exam and medical history: assessment (symptoms, family history, smoking history, exposure to environmental irritants)
Spirometry: It will show a reduced FEV1 (more severe than in chronic bronchitis), FVC and FEV1/FVC.
Imaging studies
chest X-rays: for ruling out other conditions, especially cardial; high-resolution computed tomography
(HRCT): for precise assessment of structural changes associated with emphysema, e.g. hyperinflations and bullae (air pockets).
TREATMENT
Medications: bronchodilators (for airway relaxation); steroids (in case of inflammations); antibiotics (for fighting respiratory infections, e.g. pneumonia, flu or acute bronchitis)
Vaccines: flu and pneumonia vaccinations are recommended
Pulmonary rehabilitation: combines education (nutrition, breathing techniques, help with smoking cessation) and physical exercise
Oxygen therapy: in later stages, also for home use
Surgery: lung volume reduction, damaged tissue removal
Lung transplant
Protein therapy: infusions of AAT in case of genetic AAT deficiency
Cystic fibrosis
Cystic fibrosis (CF) is the most frequent autosomal recessive disease (i.e. passed from parent to child) in the Caucasian population. It occurs in approximately 1 between 2500 and 3500 births. It is less frequent in other ethnic groups. [49]
CAUSES
CF is caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. These mutations affect the functioning of the CFTR protein, responsible for regulating the movement of salt and water in and out of cells. The defective CFTR protein leads to the production of thick, sticky mucus in various organs, primarily affecting the lungs and the digestive system.
SYMPTOMS
They usually appear at or soon after birth, most often as poor weight gain and respiratory infections.
DIAGNOSTIC METHODS
If cystic fibrosis is in the family history, carrier testing (blood or mouthwash test) for the faulty gene is advisable before pregnancy. Tests for CF can also be done during pregnancy, but are only performed in cases with high likelihood of CF as they entail risks. Cystic fibrosis can also be diagnosed in newborn screening (blood check for abnormal levels of certain substances). In the case of positive screening result, a chlorine sweat test is performed. This is the definite test for CF – elevated chlorine levels show its presence.
It is vital that the diagnosis be made as early as possible; a few weeks after birth is already too late for optimum outcomes.
TREATMENT
Pharmacogenomic treatment involves tailoring drug therapies based on an individual’s genetic makeup. However, different CFTR mutations have a different effect on the CFTR protein; this means that these medicines can only be used to treat patients with certain CFTR mutations. [51]
Treatments for CF focus on help with mucus thinning, improving digestion and breathing as well as prevention and treatment of infections. They involve airway clearance techniques (clearing mucus out of the lungs), medication (mucus-thinning drugs; antibiotics for infections; anti-inflammatory medications; pancreatic enzyme supplements for pancreatic insufficiency) and lung transplants.
BRONCHIECTASIS
Bronchiectasis is a progressive chronic condition characterised by the irreversible dilation and scarring of the airways, leading to the accumulation of mucus and recurrent respiratory infections. (In contrast, conditions like COPD and asthma are primarily marked by airflow limitation due to inflammation, narrowing of the airways, and structural changes in the lungs.)
CAUSES
Bronchiectasis may occur if the elastic tissue and muscles around the bronchi (airways) get permanently damaged; as a result, the bronchi get abnormally widened. In half of the cases, the cause is not known. [53]
Other causes include:
lung infections in childhood (measles, severe pneumonia, tuberculosis, whooping cough) in one third of cases
immunodeficiency (genetic, HIV)
cystic fibrosis
abnormalities in cilia (hair-like structures lining the airways in the lungs), caused by conditions like primary ciliary dyskinesia (genetic) and Young’s disease (affects males only, presumably due to mercury exposure in childhood)
aspiration (stomach contents accidentally passing into the lungs)
allergic bronchopulmonary aspergillosis (ABPA): allergy to aspergillus (a type of fungi)
inflammations in other areas of the body (e.g. due to Crohn’s disease, ulcerative colitis, rheumatoid arthritis)
SYMPTOMS
The permanent damage to the airways due to bronchiectasis can lead to: [52]
Mucus accumulation and therefore chronic cough with large amounts of sputum on a daily basis.
Coughing up blood.
Frequent respiratory infections (pneumonia, bronchitis).
Shortness of breath and difficulty breathing, especially during physical activity.
Persistent fatigue and lack of energy.
Chest pain or discomfort, often due to coughing or breathing problems.
Clubbing of the fingertips: due to the reduced amount of oxygen in the blood, the tissue beneath the nail thickens, giving the fingertip a bulbous appearance.
DIAGNOSTIC METHODS
The diagnosis typically involves a comprehensive evaluation that may include a detailed medical history, blood tests (to check for infectious agents – viruses, bacteria or fungi), imaging tests (HRCT – for checking the width of the airways), sputum cultures (to check for infectious agents), bronchoscopy (looking into the lungs with a camera, usually when suspecting aspiration) and spirometry. [54]
TREATMENT
Bronchiectasis causes permanent damage, but treatment can help prevent the illness from worsening. This often involves a combination of airway clearance techniques (mucus removal), medications (antibiotics, antiviral drugs), vaccinations (anti-flu; pneumococcal against pneumonia) and lifestyle modifications (exercise, hydration, balanced diet). Surgeries are rare. [55]
Restrictive conditions
Restrictive conditions reduce the lung volume, which prevents the lungs from fully expanding when the patient breathes in. They appear a lot less frequently than obstructive illnesses. In initial medical assessment, spirometry helps differentiate between these two types of conditions. [56][21]
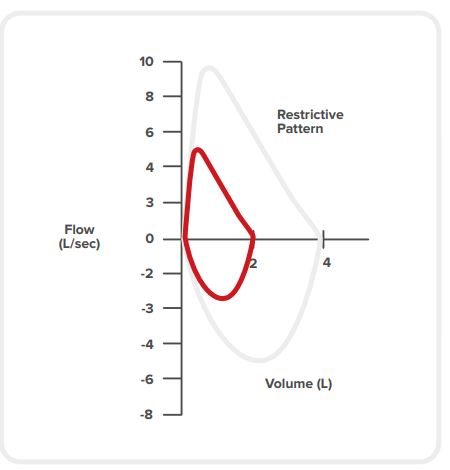
Restriction is characterised by: [11] [4]
a normal looking shape on spirometry trace, but smaller in size
reduced FVC
normal-to-high FEV1/FVC ratio (stiff lungs have an elastic recoil, which makes it easy to breathe out)
possibly a relatively high PEF
Restrictive lung conditions are caused by pulmonary or non-pulmonary factors. Pulmonary causes of restrictive lung conditions originate within the lung tissue or the airways (resulting in e.g. pulmonary fibrosis, pneumonitis). Non-pulmonary causes originate outside the lungs (e.g. aspiration pneumonia).
Pneumonitis
Pneumonitis is a broad term for lung tissue inflammation. It can also cover pneumonia as an infectioninduced inflammation. In medical practice, however, the term ‘pneumonitis’ is mostly used for noninfectious causes of lung inflammation. This condition typically arises when the lungs are exposed to an irritating substance. This causes inflammation in the tiny air sacs of the lungs (alveoli). This hinders the passing of oxygen through them into the bloodstream. [57] [58]
If pneumonitis is undetected or untreated, it may deteriorate into chronic pneumonitis, which can lead to lung scarring (pulmonary fibrosis – a life-threatening condition).
CAUSES
In most cases, the cause of pneumonitis is not identified. Frequent causes include:
Drugs, including certain antibiotics, chemotherapy medications, and those regulating heartbeat.
Airborne irritants. This can happen in farming (pesticides, moldy hay) as well as with the use of humidifiers or hot tubs (where mold can spread as mist due to vaporisation).
Bird feathers and excrement (e.g. in poultry farming or pigeon keeping).
Radiation treatments, either of the chest or the entire body.
SYMPTOMS
The most common symptom is shortness of breath with a dry cough. This can be accompanied by fatigue and loss of appetite, followed by unintentional weight loss.
DIAGNOSTIC METHODS
The first step is to find whether the patient has been exposed to any irritants that can cause pneumonitis. This involves looking at medical history and carrying out a physical exam. Further exams may include:
spirometry for lung function assessment
oximetry
blood tests to establish the level of white blood cells
CT scans or X-rays (checking for inflammation or fluid in the lungs)
bronchoscopy, which can involve lung biopsy (collection of lung tissue sample) or BAL (bronchoalveolar lavage, i.e. collection of lung fluid sample)
TREATMENT
The best treatment it is avoiding the irritant. Depending on the seriousness of the inflammation and potential fibrotic changes, the treatment can involve:
immunosuppressants,
corticosteroids,
pulmonary rehabilitation,
antifibrotic medications,
oxygen therapy or
lung transplant.
Pulmonary fibrosis
Pulmonary fibrosis causes the scarring of the interstitial tissues, i.e. cells located between blood vessels and other structures in the lung. This causes breathing difficulties. The most common form is idiopathic pulmonary fibrosis (IPF), i.e. with an unknown cause. [59]
Pulmonary fibrosis can lead to a number of complications, including respiratory failure, right heart failure and lung cancer. [57] The average survival rate is between 3 and 5 years from the time of the diagnosis. [60]
CAUSES
In most cases, the cause of pulmonary fibrosis is unknown. Its identifiable causes fall into five categories: [62] [59]
Drug-induced: chemotherapy medications, certain antibiotics, some heart medications
Radiation-induced: radiation therapy as part of cancer treatment
Environmental: smoking increases the likelihood of the disease
Autoimmune: rheumatoid arthritis, viral infection
Occupational: regular exposure to chemicals and other harmful substances (metal workers, hairdressers, farmers, stone cutters)
SYMPTOMS
Signs and symptoms of pulmonary fibrosis can appear early or take years. Persistent breathlessness (dyspnea) is the most common problem. Others include a dry cough, fatigue, unexplained weight loss, muscle and joint ache, clubbed fingers and toes (due to insufficient oxygen in the blood). [61]
DIAGNOSIS
Pulmonary fibrosis shares many symptoms with other lung conditions, which make it difficult to diagnose. The following methods are used for diagnosing it: [59]
Blood tests: to rule out other illnesses and monitor disease progression.
Imaging tests: a picture of lung scarring can help confirm the diagnosis. Chest X-rays or CT scans are used.
Pulmonary function tests
Oxygen desaturation study: for measuring oxygen levels in the patient’s blood during various activities.
Lung biopsy: taking a sample of lung tissue for analysis.
TREATMENT
There is no cure for the condition. Most pulmonary fibrosis treatments focus on easing symptoms, slowing the scarring process and improving the patient’s quality of life. [59] [61]
Medication: antibiotics, corticosteriods
Ventilator: for acute exacerbations (rapid symptom worsening)
Oxygen therapy
Pulmonary rehabilitation
Lung transplant
Sarcoidosis
Sarcoidosis is a multi-system disease characterised by an overreaction of the immune system, which leads to an inflammation pattern termed granulomas (nodules of immune cells that form because the immune system tries to wall off foreign substances that it can not eliminate). It can appear in any organ, including the lungs, and affects its functioning. It can occur regardless of age or ethnicity. However, Scandinavians (compared to other Caucasians) and African Americans have a higher incidence. 70% of cases occur between the ages of 25 and 40; a second peak appears to be in women over 50. [63] [64]
CAUSES
The exact cause of sarcoidosis is not known. There might be a genetic predisposition, which could be triggered by environmental factors like viruses, bacteria, chemicals or dust. [64]
SYMPTOMS
The symptoms of sarcoidosis depend on the organ affected. In the lungs, it is characterised by respiratory symptoms, cough, chest pain and dyspnea. [63]
DIAGNOSTIC METHODS
If sarcoidosis is suspected, a lung CT scan or a chest X-ray will be performed. Sometimes, bronchoscopy together with biopsy (taking a sample of lung tissue) can be used. [65]
TREATMENT
Often, the disease disappears without treatment in a few months or years. Non-prescription painkillers (e.g. ibuprofen, paracetamol) are used for pain episodes. With more serious complications, steroid pills are used to relieve pain, reduce inflammation and prevent scarring. [65]
Read more about How to conduct a spirometry measurement
Read more about Automatic tools in spirometry

Learn how to successfully perform spirometry in a comprehensive e-book where we cover:
- How spirometry works
- How to conduct a spirometry measurement
- Frequently diagnosed conditions
- Automatic tools in spirometry
- A comparison of different spirometry devices
- Technical specifications of the MESI mTABLET SPIRO
